
Interview with Dr. Deb Houry, Former CDC Chief Medical Officer and Deputy Director for Program and Science, Emergency Medicine Physician, Adjunct Professor
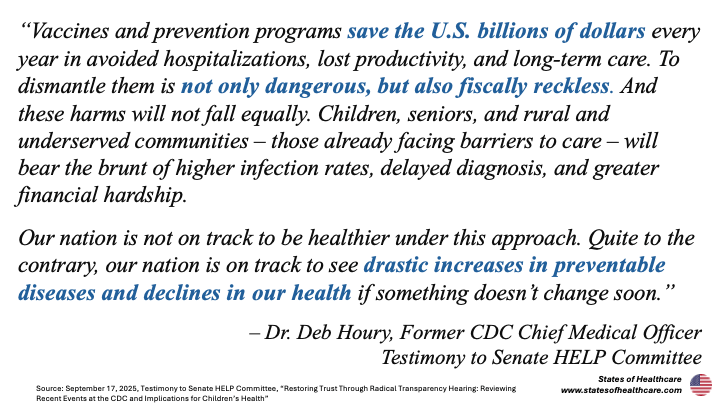
“I am concerned about the future of the CDC and public health in this country given what I have seen. If we continue down this path, we are not prepared – not just for pandemics but also chronic disease – and we are going to see kids dying of vaccine-preventable illnesses
– Dr. Deb Houry, MD, MPH
An Emergency at the CDC
Dr. Deb Houry is well-acquainted with emergencies.
After earning bachelor’s, master’s, and medical degrees at Emory and Tulane University respectively, she began her career as an emergency medicine physician.
“My favorite place was down in the emergency room because I liked the uncertainty of what was next, and I liked being in the safety net for any patient,” she recounts.
Then after over a decade of blending emergency medicine, public health, research, and teaching at Emory University, she became the CDC’s Director of National Center for Injury Prevention and Control in 2014. There she led the CDC’s efforts to combat the opioid epidemic, rising suicide rates, and gun violence deaths. Her team developed the CDC’s clinical guidelines for opioid prescriptions and helped create a national suicide prevention strategy.
In 2021 Deb became the Acting Principal Deputy Director of the CDC. Here she co-led the agency restructuring to address lessons learned from the Covid-19 pandemic, including lab quality improvements, timely data, response readiness, and public-private partnerships.
Next Deb became the Chief Medical Officer and Deputy Director for Program and Science at the CDC in 2023. Following the 2024 election, Deb was the CDC’s transition lead – the person responsible for working with new Health and Human Services (HHS) Secretary Robert Kennedy Jr. and the Trump Administration. In her over ten years in leadership at the CDC, Deb worked with both Republican and Democratic leadership through four presidential administrations and under six CDC directors.
“I always believe in optimism and hope. I read Secretary Kennedy’s books and as the transition lead was prepared to welcome him. After seeing the number of misstatements in his Senate Finance Committee testimony, how he has asked our scientists to compromise our integrity, and the children that have died under his watch, I think he should resign,” Deb eventually testified before the Senate.
2025 in Review: A Year of Disruption at the CDC
On February 13th Kennedy was confirmed by the Senate (52-48) as the Secretary of Health and Human Services.
On June 8th Kennedy replaced all seventeen members of the CDC Advisory Committee for Immunization Practices (ACIP), the body responsible for creating national vaccination recommendations. This contradicted what he pledged to Republican Senator Bill Cassidy, who is a physician, when Cassidy confirmed him in February.
On July 29th Dr. Susan Monarez was the first CDC Director confirmed by the Senate (51-47) based on a newly enacted 2023 law.
On August 8th a man fired 500 times at the CDC headquarters in an attack motivated by his “discontent with the Covid-19 vaccine.” The shooter murdered Dekalb County Police Officer David Rose, a Marine veteran whose wife was expecting their third child, when he responded to the shooting.
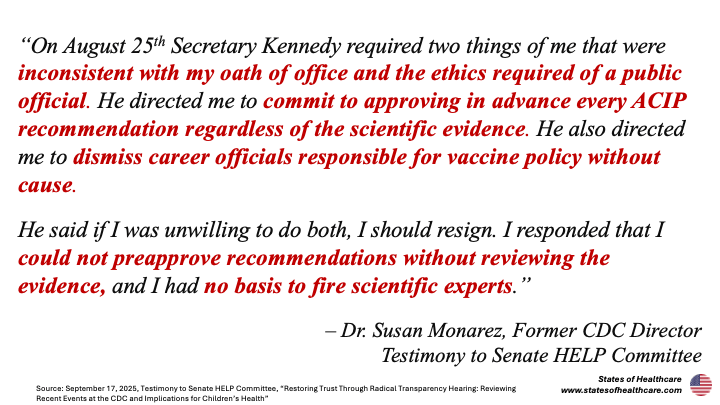
On August 25th Kennedy allegedly directed Monarez to commit in advance to approve future unknown changes to the childhood immunization schedule that Kennedy said would come from the September ACIP meeting. (The Secretary denies this.) Director Monarez also says that she resisted his direction for her to “dismiss career CDC officials responsible for vaccine policy without cause.”
On August 27th the White House fired CDC Director Monarez twenty-nine days into her tenure.
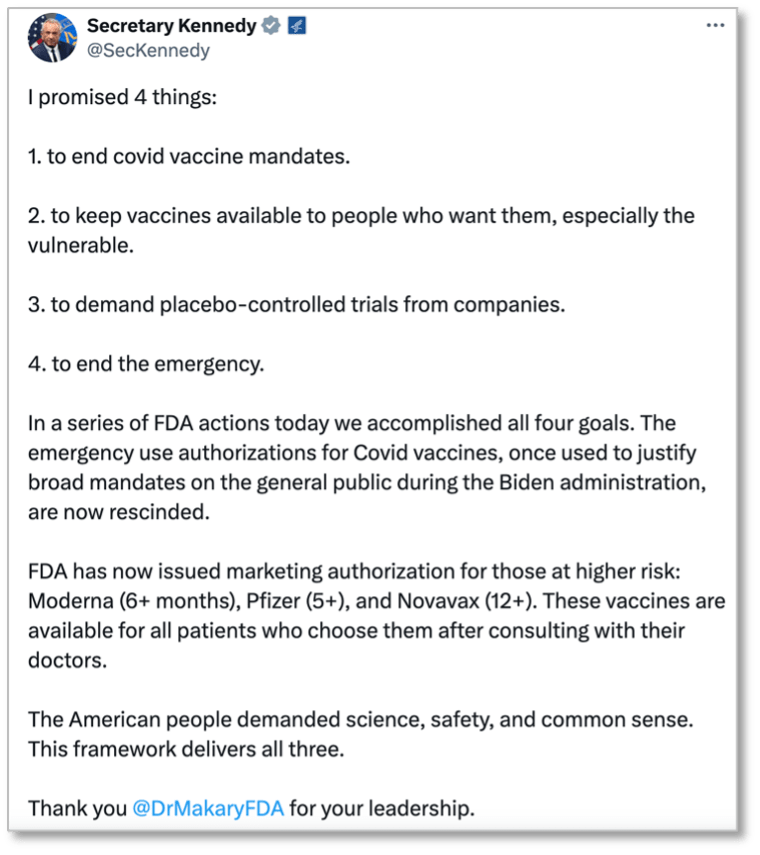
Also on August 27th, Kennedy announced via tweet that the FDA had ended the Covid-19 vaccines’ emergency use authorizations, narrowing their approved use to a smaller patient population of patients at “higher risk.”
On August 28th, in response to the firing of Director Monarez, Dr. Houry resigned and was joined by two of her direct reports, CDC Directors Daniel Jernigan (Director of the National Center for Emerging and Zoonotic Infectious Diseases) and Demetre Daskalakis (Director of National Center for Immunization and Respiratory Diseases), in a coordinated resignation. The former leaders walked out of the CDC office together to a gathering of hundreds of supporters. At the walkout, the trio spoke about the recent changes at the CDC that led them to resign and then placed flowers at an intersection memorial for Officer Rose.
“I hope this is the tipping point. I hope losing the CDC Director, us, and many others who come behind us is the tipping point. This is enough,” Deb said at the walkout. “We need to get our people back. We have to allow for independent experts.”
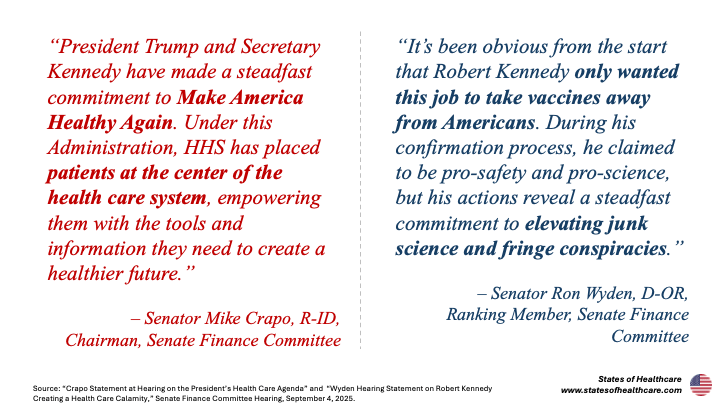
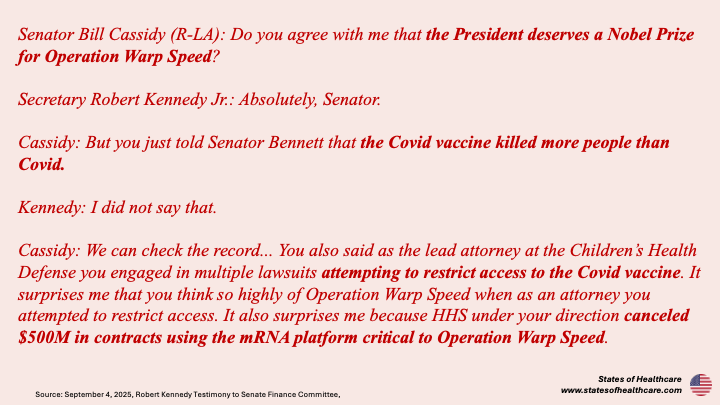
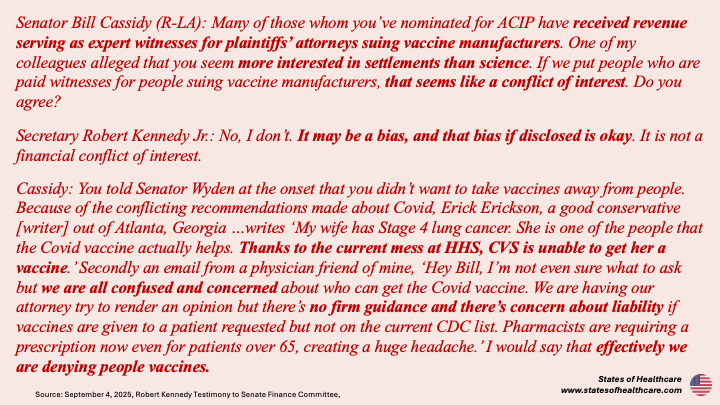
On September 4th Kennedy appeared before the Senate Finance Committee. The day prior, Dr. Houry released an op-ed in the Washington Post with several questions to ask Kennedy at the hearing. The day of the hearing Monarez released an op-ed in the Wall Street Journal about her firing. In combative exchanges, Kennedy testified before the Senate that the op-ed’s depiction of her firing was a lie.
On September 17th former CDC Chief Medical Officer Deb Houry joined former CDC Director Monarez in testifying before the Senate Committee on Health, Education, Labor and Pensions for almost three hours of sometimes heated interrogation.

Former CDC Chief Medical Officer Deb Houry testified alongside former CDC Director Susan Monarez before the Senate HELP Committee at the Restoring Trust Through Radical Transparency Hearing on September 17th. Source: Senate HELP Committee.
On December 5th Deb called for oversight of the CDC in a Time op-ed entitled “I Left the CDC 100 Days Ago. My Worst Fears About the Agency Are Coming True.”
As of mid-December when we spoke, her alarm has not abated.
“I am concerned about the future of the CDC and public health in this country given what I have seen. If we continue down this path, we are not prepared – not just for pandemics but also chronic disease – and we are going to see kids dying of vaccine-preventable illnesses,” Deb shares.
“Before this current administration, you did not completely redo the entire agency every four years or when there was a new director,’” she recounts. “Change was at a programmatic level, not a complete shift of the agency.”
“The About Us page on the CDC web page has changed. In my mind, it should always kind of look the same and be kind of boring with just data and technical information. It should have ‘We want to protect people’s health 24/7, and here’s our latest director’s priorities, and what are the leading causes of death or morbidity.’ We should be interpreting data for how it impacts health and clinical guidance – nothing else. There shouldn’t be any ideology there,” she attests.
Today the About CDC web page includes a broad swath of stances, including views on immigration, abortion, street crime, gender ideology, DEI, and parental rights over children’s educational curriculum in schools.
“I always say that we should be allowed to be data-driven, ‘nerdy’ scientists and do our jobs in the same manner regardless of who is leading. You should be able to look to the CDC and just see science,” Deb summarizes.
Deb explains that Congressional oversight of the CDC could include probes into the representation on federal advisory committees and monitor transparency, including whether the CDC posts materials and any vote language in advance of meetings so the public has enough information to give comment. Congress also questioned the number of political hires recently at CDC and should further examine this, she notes.
“There needs to be oversight into how decisions are being made and how the agency is run. And the Senate could bring the Secretary back for a follow up hearing, as they said they would after I testified,” Deb details.
While the 2025 Senate hearings were lively, they did not seem to translate to real action. Deb was initially hopefully but now does not expect Congress to act more tangibly any time soon.
“Unfortunately, for greater action I think there would need to be an outbreak that the CDC is unable to respond to or continued pediatric deaths from preventable diseases,” she states.
The Evolution of the CDC
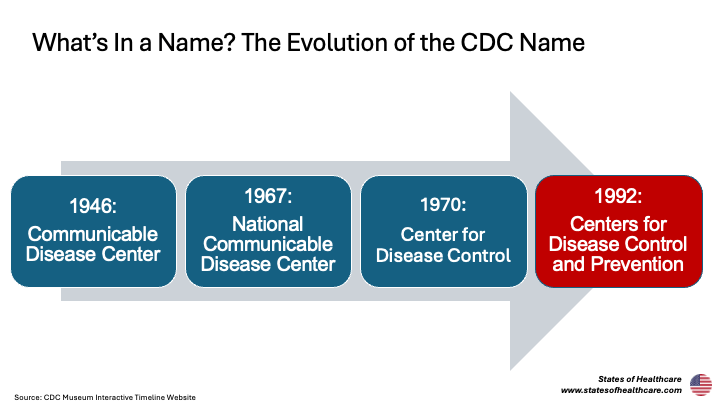
The CDC was founded in 1946 as the Communicable Disease Center and initially tasked to defeat malaria in the South (a fight officially won in 1949 – take that mosquitoes). The CDC gained its headquarters in Atlanta (metro population: 6.4M), Georgia (population: 11M) after philanthropic maneuvering from Coca-Cola chairman Robert Woodruff. It is located across the street from Emory University, a proxy that mirrors the close relationship between the organizations. With Georgia Tech nearby as well, Atlanta is well positioned as a world-class research city.
The CDC’s early purview grew to include plague suppression, veterinary public health (e.g., rabies), and disaster response. Now the CDC is the world’s premier public health institute. The agency leads the nation’s efforts to understand and intervene against causes of excess mortality and morbidity, from infectious diseases (e.g., measles, polio, tuberculosis, smallpox, rubella, H1N1) to environmental contaminants (e.g., asbestos, lead) to social determinants of health (e.g., gun violence, intimate partner violence). They serve as the nation’s frontline responders for everything from biochemical terrorism to infectious disease outbreaks to maternal mortality to overdose deaths. Approximately 80% of the CDC’s domestic budget goes to state and local health partners (i.e., Departments of Health) to support community-based public health. CDC funding comprises most of the public health funding for many states.
During the Covid-19 pandemic, primarily during the first Trump presidency, the CDC developed a laboratory diagnostic test, created the SPHERES consortium to sequence the virus’ genome, released iterations of guidelines for social distancing, and eventually created guidelines for Covid-19 vaccination.
In a September 2nd op-ed, Kennedy opined that the CDC’s “bureaucratic inertia, politicized science, and mission creep have corroded [its] purpose and squandered public trust.” In the op-ed, Kennedy noted plans to narrow the CDC’s focus back to infectious diseases, minimizing some of its broader work.
Deb does not think this is a good idea.
“Public health does not have silos. Public health is about prevention overall, and there is all this synergy with infectious and noninfectious disease. If you separate them, you lose that,” Deb explains. “Diseases like Zika or Oropouche can cause fetal abnormalities and require environmental interventions for insects. There is a linkage with HIV and Hepatitis and needle-sharing. You needed an emergency response lens that encompasses all these disciplines.”
The CDC, ACIP, and Vaccines
Much of the controversy surrounding recent efforts at the CDC centers vaccines.
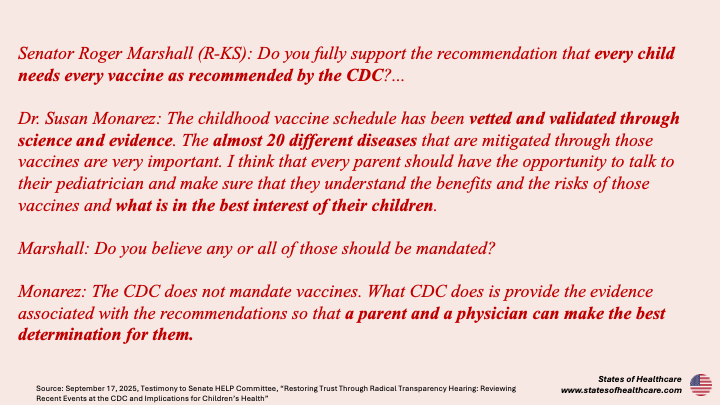
Vaccination recommendation decisions start with the Advisory Committee for Immunization Practices (ACIP), which advises the CDC on which Americans (i.e., age cohorts, health risk factors) should ideally receive which vaccinations and when. The CDC held the first ACIP meeting in 1964. The CDC Director then reviews the ACIP recommendations and can choose whether to adopt them as the “Standards of Care” to advise clinicians nationally. The CDC does not create any vaccine mandates. Certain states and localities set vaccine mandates for school attendance, but these as well as insurance coverage are typically informed by CDC recommendations.
Prior to 2025, ACIP assessments were carried out in the same systematic manner.
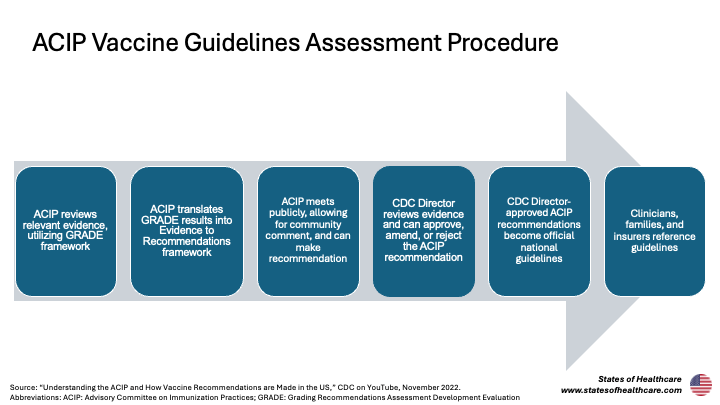
The ACIP typically organizes evidence into a framework called GRADE: Grading Recommendations Assessment Development Evaluation. Deb explained to me that GRADE is a system that assigns value to types of evidence, weighting on a spectrum with randomized controlled trials highest and anecdotes lowest. The GRADE system directs the committee to focus on the highest quality evidence. Deb notes that this process was omitted in the recent 2025 ACIP meetings.
The ACIP translates results from the GRADE assessment into the Evidence to Recommendations framework, which considers the balance of benefits and risks, quality of evidence, preferences of the patient population in question, and a health economics analysis. Again, Deb notes that this essentially stopped in recent meetings.
ACIP decisions are determined at public meetings, which invite citizen comment.
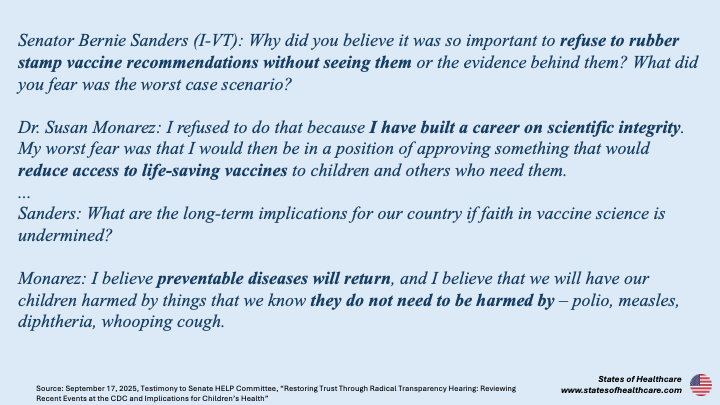
Typically, once the ACIP makes a recommendation, the CDC Director is tasked with approving, amending, or rejecting it based on the evidence. Former CDC Director Monarez testified before the Senate HELP committee that she was fired for her refusal to “commit in advance to approving every ACIP recommendation regardless of the scientific evidence” ahead of the September ACIP meeting.
CDC Director-endorsed ACIP recommendations are considered the official, up to date vaccination guidelines for the nation.
The ACIP also typically requires that all members disclose any conflicts of interest; these are published on a public database that goes back to 2000 and notably excludes the 2025 appointments.
Gold Standard Science
The phrase “gold standard science” appeared frequently in 2025 political discourse. In May, President Trump enacted the Restoring Gold Standard Science Executive Order. The order describes gold standard science as “reproducible, transparent, communicative of error and uncertainty, collaborative and interdisciplinary, skeptical of its findings and assumptions, structured for falsifiability of hypotheses, subject to unbiased peer review, accepting of negative results as positive outcomes, and without conflicts of interest.”
However, all that glitters is not gold.
“I too believe in gold standard science. Unfortunately, we are not currently seeing that at the CDC,” Deb highlights. “At the most recent CDC vaccine committee meeting they had people that had potential conflicts of interest and presenters with retracted scientific papers. Anecdotes were given the same weight as a randomized clinical trial. At the prior meeting, they presented on vaccines that were not in the United States in a discussion about an American vaccine. These are examples for me where what was presented was not the best evidence.”
For anyone trying to decipher fact from fiction in the age of misinformation, regardless of your training and background, Deb has some helpful guiding questions: where, what, and how.
First, she advises anyone trying to interpret evidence to ask where it is from.
“Where did the science come out? Did it come out in a peer reviewed journal, or is it a social media post? If so, drill down below and see if where the science comes from, like the Journal of the American Medical Association, New England Journal of Medicine, or the CDC’s Morbidity and Mortality Weekly Report,” she suggests. “The evidence should be from a reputable peer reviewed journal.”
Then, consider what, or the type of evidence, considering that certain types are more valuable.
“Is it a personal anecdote, somebody’s experience, or is it a clinical trial?” she asks.
Finally, consider how the evidence was gathered.
“What was the actual study design? Is it transparent on how the analyses were done and can someone replicate them?” she explains.
On January 5, 2026, the CDC dramatically revised the childhood immunization schedule, narrowing the routine recommendation from protecting against 17 diseases to 11. This change was made from a decision memorandum from the current acting CDC director and was not reviewed or endorsed by the ACIP.
“This decision commits NIH, CDC, and FDA to gold standard science,” NIH Director Jay Bhattacharya opined in the HHS press release.




Leave a comment