
Interview with Clare McNutt, Physician Associate, Mental Health Policy Research Leader, Assistant Professor
“Several times a month, I have friends reach out who are desperate for help navigating mental healthcare for a loved one. It is heartbreaking to face the reality that, despite my deep connections and expertise in this field, I often have no choice but to tell them their only option is the hospital. The fact that even with my network and insider knowledge, I struggle to find timely care is a stark reminder of how deeply flawed our system is and why I remain committed to this work.”
– Clare McNutt
The Emergency of Behavioral Healthcare
When Clare McNutt took a position in an Emergency Department (ED) as a newly graduated Physician Associate, it was partly because she did not want to specialize in mental healthcare yet.
Physician Associates (PAs), sometimes referred to as Physician Assistants, are licensed clinicians with a master’s degree in PA Studies who provide medical care across a variety of healthcare settings in collaboration with physicians.
“I was always fascinated by mental healthcare, but I didn’t want to go straight into psychiatry because part of the beauty of being a PA is you are not forced to immediately specialize. I was convinced that emergency medicine was the place to go to hone my skills more broadly and better understand my strengths,” Clare explains.
However, Clare soon learned that many patients rely on the ED for basic mental healthcare.
“In the ED, it felt like I was seeing the same twenty-five patients with mental health needs multiple times per week and that led to a lot of soul searching for me. I was wondering what in the world is wrong with the system at large that these folks have to come to me to get their psych meds,” she recalls. “I kept thinking that this cannot be the way that things are supposed to be.”
Folks concerned with American healthcare spending have long tried to pinpoint the prevalence and drivers of patients who frequently visit the ED, sometimes referred to as ED recidivists, with the hope of devising interventions to funnel patients to cost-efficient venues for care. A 2018 study found that in California in 2014-2015, 8.5% of ED patients visited the ED at least four times a year and accounted for 31.6% of all ED visits. Mental health diagnosis was found to be one of this patient group’s largest predictors.
In her self-described naivety, Clare thought that her frequent visitor patients with mental health illnesses were likely not receiving strong discharge plans from inpatient psychiatric stays, causing them to seek regular help from the ED. After three years working in EDs across DC, Maryland, and Virginia (colloquially referred to as the DMV), she transitioned to an inpatient psychiatric hospital in the hopes of working on this issue.
She spent the next five years caring for patients with mental illness but also trying to deeply understand a hopelessly fragmented healthcare system.
“There are never enough folks delivering care in the mental health field,” she reflects. “My work included evaluating how we staffed nurse practitioners and PAs with psychiatrists so we could see consults faster, spend more time with patients on the units, have time to call patient families, and speak to the patient’s outside psychiatrists to make sure we were are on the same page about the medications that the patient was going to leave on.”
Like many physician specialties, psychiatry faces a shortage. The Health Resources and Services Administration (HRSA) has predicted a shortage of 12,000 psychiatrists in the US by 2030. The average age of American psychiatrists is fifty-five and few new physicians are entering the specialty. Staffing patterns like the one Clare described lean on additional advanced practice clinicians to stretch clinical capacity and coverage. The regulated scope of practice for PAs and nurse practitioners (NPs) varies by state, but in Maryland both clinician types have some level of prescribing power, which also supports their work in psychiatry.
After being on call five nights a week and caring for patients in two to three hospitals across Maryland daily, Clare was still passionate about mental healthcare but exhausted. Like many healthcare workers, she wanted out of the hospital.
Mental Healthcare Delivered from the Primary Care Office
As Clare searched for a new position, she found an opportunity to join a mental health tech startup, based in Silver Spring, Maryland, with a platform to implement a relatively new framework for mental healthcare delivery called the Collaborative Care Model,
[If Silver Spring (population: 82,000) rings lyrical bells, the Rumours are true: it was the titular inspiration behind the electrifying and similarly named Fleetwood Mac breakup anthem after Stevie Nicks noticed the city name while traversing the Maryland highway on tour.]
“The Collaborative Care Model integrates mental healthcare into the primary care space. It has a vast evidence base of impressive clinical outcomes and focuses on identifying patients with mental health needs earlier in their trajectory, hopefully preventing the need for emergency care or inpatient stabilization,” Clare outlines. “Enabling access to evidence-based care where the patient was already being seen and that could be billed to the patient’s medical benefit seemed like a winner.”
Since the Collaborative Care Model (CoCM) was developed at the University of Washington in the 1990s, more than ninety randomized clinical trials and meta-analyses have evaluated how the model impacts clinical outcomes in depression, anxiety, and other mental health conditions.
In many situations, primary care is the only contact patients have to the healthcare system. Barriers to specialized mental healthcare include provider shortages, high out of pocket cost, and social stigma.
CoCM leverages an interdisciplinary care team to monitor and treat mental health needs through primary care. A behavioral health care manager (BHCM) liaises with the primary care provider (PCP) and supports the psychiatric consultant. The BHCM collaborates with the psychiatric consultant weekly through a systemized review of each patient on their panel, utilizing a data-driven registry platform. The psychiatric consultant then provides recommendations for any treatment adjustments necessary to help patients reach their clinical targets, and the BHCM reports these back to the PCP for implementation. The BHCM meets routinely with the patient, assesses their progress using validated tools, and delivers brief therapeutic interventions.
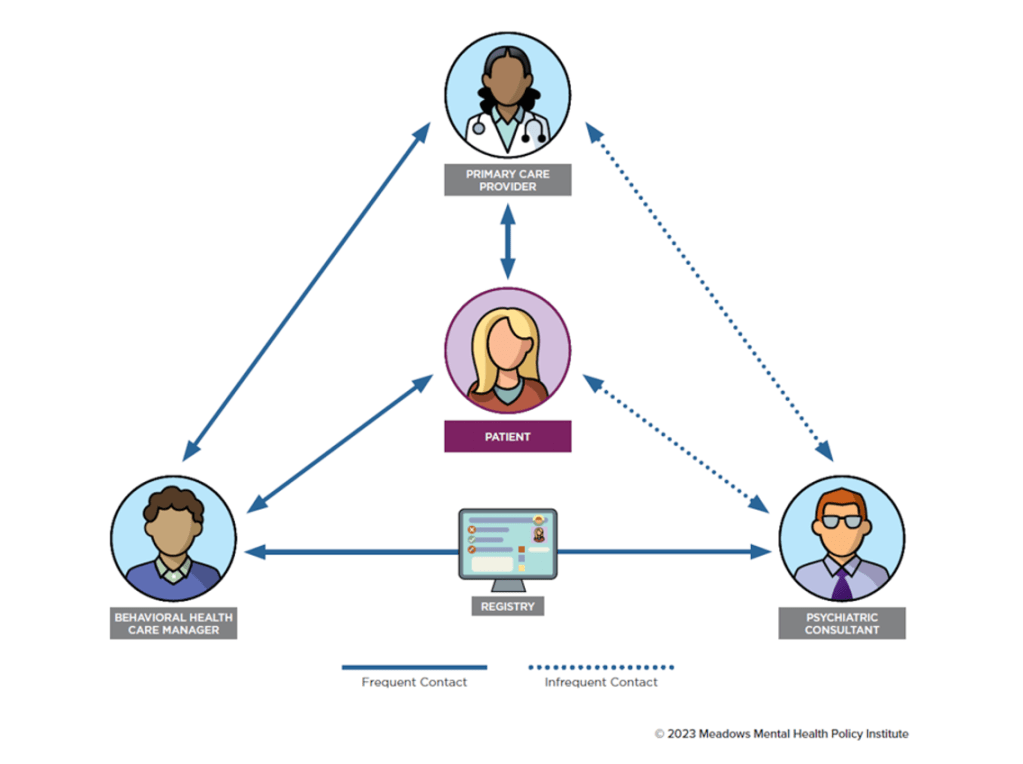
CoCM provides psychiatric care from a team of complementary providers.
Source: “Collaborative Care Model: An Overview,” Meadows Mental Health Policy Institute, 2023.
“Patients like the model because they can stay connected with their PCP and don’t have to call a bunch of numbers to see if a mental health clinic takes their insurance and has an appointment available in the next 90 days,” Clare shares.
During her five year tenure, Clare helped expand the CoCM program from one Maryland pilot clinic to sites across seventeen states.
“We found clinics that were willing to take a chance on an innovative model and because of their belief in the importance of making quality mental healthcare available to all, the state of Maryland extended the benefit to all folks with Maryland Medicaid,” she recalls. “We showed that CoCM helps patients clinically, that patients and providers are happy, and that Medicaid can afford to reimburse it.”
Many patients and clinicians are skeptical of mental health apps, especially after the apparent boom and bust of many during the COVID years.
“I understand the fear of losing human connection since so much of what can perpetuate mental illness symptoms has to do with isolation and a lack of connection. I get where people are wary of using machines for care,” Clare reflects. “We really have to consider technology as a way to support what humans do for humans and not as a way to replace what humans do for humans, but I think technology can be incredible asset to increasing access to care.”
One way Clare identifies technology as a boon in the mental health space is how it can increase access to measurement informed care.
CoCM emphasizes continually measuring outcomes via validated survey tools. The model also encourages universal mental health screening – completing basic mental health assessments during annual physicals to identify if a patient needs mental health intervention. Once a patient is diagnosed with a mental health condition, these tools measure symptom progression and treatment effect. Per CoCM, clinicians adjust treatment plans, based on the results of these monthly validated assessment tools, patient preference, psychiatric consultant recommendations. and psychiatric. Treatment plans include lifestyle changes, brief therapeutic interventions and/or medication, and adjustments continue until the patient achieves at least a 50% reduction in symptoms.
“In behavioral healthcare, we need to quantitatively assess progress just like they do in any other part of healthcare. You would never go to your PCP and expect them to adjust your treatment plan without checking your blood pressure or blood sugar and looking at those numbers,” she explains. “We need to track progress for mental health symptoms too. Enabling patients to fill out assessments virtually through apps or patient portals can increase engagement and help us track outcomes better.”
From the Hospital to Capitol Hill
“I sometimes joke that PA school is a bit like learning to be a mechanic. I learned about differential diagnosis, organ systems, and how to take care of the human body like a car,” Clare reflects. “Maybe I was so overwhelmed by the sciences, but I didn’t pay attention to the American healthcare system or policy. It sounds naïve but I was just focusing on the patient at the time.”
As she learned more about the mental health policy landscape through her career, it struck her how health policy was not stagnant but something that could be shaped for the betterment of patient care.
Now Clare’s career bridges her clinical and policy expertise. She currently serves as the Senior Vice President for Health System Integration at the Meadows Mental Health Policy Institute, which includes integrated care and specifically CoCM as one of its focuses. She also is an assistant professor for her alma mater George Washington University’s PA program and an affiliate faculty member at the University of Texas at Austin. Currently, she is completing an executive doctoral program at her undergraduate alma mater, the University of North Carolina at Chapel Hill in health policy and management to further hone her knowledge of the healthcare system at large. Her role at the Texas-based Institute and UT Austin are also remote, allowing her to remain in her beloved Maryland neighborhood.
Clare’s location in Maryland also supports policy engagement. She joined a team from Meadows on Capitol Hill to express support for the Complete Care Act, a 2023 bill (just introduced in the House in March 2025) to adjust Medicare reimbursement to incentivize the expansion of CoCM. Clare’s policy engagement is motivated in part by her understanding of the downstream stakes of mental health policy.
“Several times a month, I have friends reach out who are desperate for help navigating mental healthcare for a loved one. It is heartbreaking to face the reality that, despite my deep connections and expertise in this field, I often have no choice but to tell them their only option is the hospital,” she reflects. “The fact that even with my network and insider knowledge, I struggle to find timely care is a stark reminder of how deeply flawed our system is and why I remain committed to this work.”
Maryland: Advocacy, Shared Values, and Innovation
Like many of her Maryland (population: 6.3M) neighbors, Clare moved slightly north from DC (population: 680,000) to Bethesda (population: 67,000) when she and her husband expanded their family. Bethesda and adjoining Chevy Chase (population: 9,500) contain all the benefits of community-based suburbia with an easy commute to the nation’s capital city. Baltimore (population: 565,000), Maryland’s biggest city, also is only an hour away.
“I think Maryland is pretty underrated by some,” Clare muses. “I wonder if they know that from where I live in Maryland you can be in DC in two minutes, at the beach in three hours, and to the mountains to ski in two hours?”
While this has evolved significantly, especially with the rise of remote work post-COVID, in 2000, 18% of working Marylanders commuted out of state to their jobs. Many of these commuting (or telecommuting) Marylanders work in government, which bleeds into the state’s culture.
“People in Maryland, especially near me, are really active and involved in local and statewide policy,” Clare describes. “This is not a state where people rest on their laurels, and I love the amount of advocacy. I love that it reflects how people here don’t take for granted that their ideals are reflected in the state government – they actively make sure they are.”
Keeping with the state’s politically engaged culture, Maryland pioneers innovative health policies. In 1977, Maryland became the first state to gain a waiver from the Centers for Medicare and Medicaid Services. This allowed the state to institute that Medicare, Medicaid, commercial insurance plans, and uninsured (i.e., self-pay) patients all pay the same prices for hospital services, which are set by an independent state agency. Typically, commercial plans pay higher rates, which can both cost these patients more and incentivize hospitals to treat more commercial patients and fewer Medicaid patients to remain financially stable.
This all-payer model, now called the total cost of care model, has been refined in several iterations that have introduced financial risk sharing mechanisms for hospitals and care coordination incentives across settings of care. From January 2014 to June 2018, the model lowered Medicare spending in Maryland by an estimated $1B. To complicate matters, a CMS review of the model also highlighted that despite model savings, Maryland still had the highest per capita Medicare spending in the nation in 2018 when CMS weighted beneficiaries in other states to match Maryland’s demographic and health status data (unweighted, Maryland ranked seventh). In 2020 Maryland had the tenth highest per capita Medicare spending in the nation, unweighted.
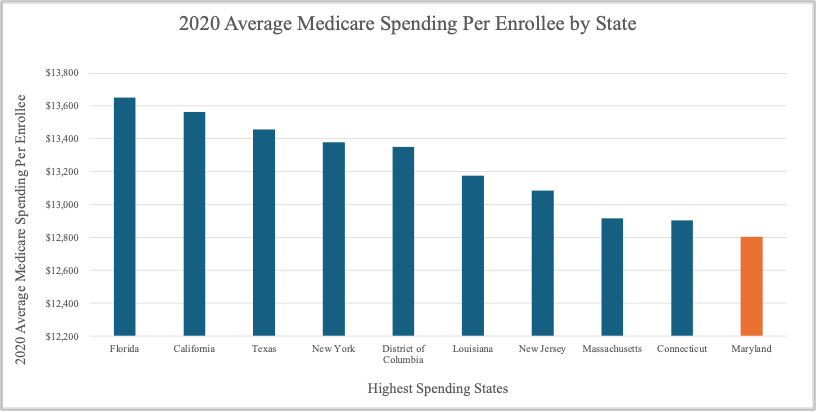
In 2020, Medicare spent an average of $12,805 per Medicare enrollee in Maryland.
Source: National Health Expenditure Data, CMS. Health Expenditures by State of Residence: summary tables.
Maryland’s total cost of care model, alongside two other models, inspired the creation of the new CMS AHEAD model, which Maryland is slated to pilot alongside five other states in 2026. The model aims to contain healthcare spending while promoting health equity.
“In Maryland we have more options for healthcare versus other states, but I want the most access to the best healthcare for everyone, not just for Marylanders,” Clare summarizes. “I think we as a state need to be at the forefront of financially incentivizing health and disease prevention rather than healthcare usage which is really just sick care.”






Leave a comment