
Interview with Mark Cuban, Entrepreneur, Co-Founder of Mark Cuban Cost Plus Drugs and Cost Plus Wellness, Former Shark, Partial Owner of Dallas Mavericks
“Nobody in this country looks at the economics of healthcare and says, boy, this is the right way to do it. They might like their doctor, and they might like the care they get. We’ve been able to push science to solve things that we never imagined we could cure. But when you look at the economics, it’s a mess.
And it’s a mess mostly because it’s dominated by just a few companies, and they’re completely opaque. As an entrepreneur, that is a ripe opportunity to change things.”
– Mark Cuban
Mark Cuban’s Journey to the Center of American Healthcare
To say that Mark Cuban receives a lot of business pitches might be an understatement. Many have come through television show Shark Tank, where Mark famously served as an investor from 2011 to 2025, but a surprising amount ends up in his inbox. In 2018, Mark received one of these cold email pitches from Dr. Alex Oshmyansky, a radiologist-turned-entrepreneur who had created a public benefit company offering affordable generic medicines.
In 2022, the two cofounded Mark Cuban Cost Plus Drugs, a public benefit company with a transparent pricing model. For each medication, the company sets the price based on the exact manufacturing costs, a 15% mark-up, a pharmacy dispensing fee ($5 for most generics), and a shipping fee ($5.25 for most generics). The Cost Plus Drugs website lists each price component publicly for every product.
“If you look at Cost Plus Drugs, we have the same price for everybody, and we’re completely transparent about that. When our costs go down, our price goes down. That tells everybody how we see pricing,” Mark explains.
Cost Plus Drugs offered around 100 generics at launch and today sells around 4,000 different medicines, including generics, biosimilars, and some branded originator drugs.
On the surface, Cost Plus Drugs is primarily a company that sells generic drugs directly to consumers online. However, the business hoisted Mark deep into the very tangled and anything-but-transparent healthcare ecosystem. That led Mark to expand his focus, to not only offer affordable generics but positively disrupt the other aspects of healthcare that he encountered that were rigged against patients, clinicians, and employers.
“Nobody in this country looks at the economics of healthcare and says, boy, this is the right way to do it. They might like their doctor, and they might like the care they get. We’ve been able to push science to solve things that we never imagined we could cure. But when you look at the economics, it’s a mess,” he emphasizes. “And it’s a mess mostly because it’s dominated by just a few companies, and they’re completely opaque. As an entrepreneur, that is a ripe opportunity to change things.”
These days, Mark spends 90% of his entrepreneurial energy on healthcare. His healthcare advocacy resembles evangelizing at times as he tries to convince all types of decisionmakers, from company human resources leads to Fortune 500 CEOs to major politicians, to break inertia and make a change toward a better, transparent state.
Much of his advocacy collapses into three key messages (if you are particularly Shark Tank-inclined, perhaps think of them as pitches):
- America pays too much for prescription drugs
- American employers overpay for healthcare
- Mobile manufacturing is the next big thing
America Pays Too Much for Prescription Drugs
Prescription drugs account for about 10% of healthcare costs in America.
In America, the cost of prescription drugs is heavily influenced by pharmacy benefit managers (PBMs). PBMs negotiate with pharmaceutical manufacturers on behalf of health insurance plans, hypothetically leveraging their volume (aka covered lives) to obtain better deals on drugs. PBMs then control access to prescription drugs by setting which drugs are listed on their formulary, a list of all drugs available for members of a plan. They further manage access through something called utilization management, an umbrella term for gatekeeping tactics like prior authorization and step therapy (sometimes called fail first).
On paper, the goal of PBMs is to lower drug prices for health plans. In practice, they do not always fulfill this goal.
If you ask someone in pharma why drug prices are so high, they will likely blame PBMs (just ask PhRMA). If you ask someone at a health insurance plan or PBM, they will likely blame pharma (just ask AHIP).
“Whoever controls the customer has the most leverage,” Mark asserts.
In 2025, the three largest PBMs (CVS Caremark, Optum, and Express Scripts) processed 80% of the country’s prescription claims. These three PBMs are subsidiaries of companies that own major insurers (Aetna, UnitedHealthcare, and Cigna), creating complicated financial incentives for these vertically integrated behemoths (which own even more components of the healthcare supply chain as mapped here).
“If there were no formularies associated with PBMs, then we could have a discussion that maybe the branded drug manufacturers have leverage, because they set the pricing. But the way it stands right now, there’s just no question that all the leverage is on the side of the vertically integrated companies, the insurance carriers slash PBMs,” Mark assesses.
PBMs often obtain their lower prices from manufacturers in the form of rebates, where the drug manufacturer pays back the PBM a confidential sum after the drug purchase is complete.
“When people think about rebates, they think about the complexity and the misallocation of those rebates. But the thing about rebates is that they distort the pricing between brand manufacturers and distributors,” Mark explains.
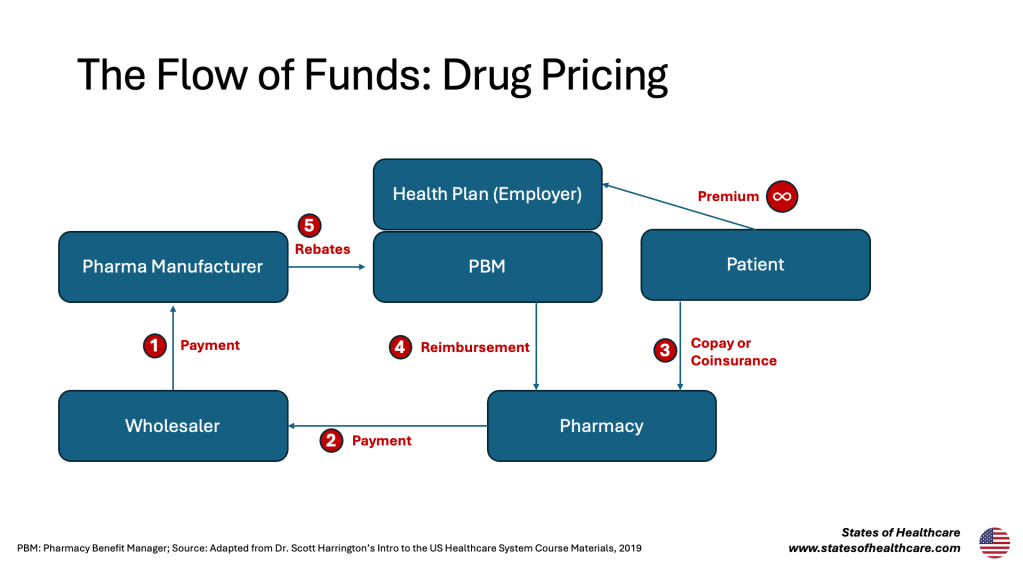
Mark argues that rebates ultimately inflate the price of drugs within the distribution supply chain, making it impossible for pharmacies to sell the product at a lower price. Maximizing the payment in Step 1 in the figure above keeps the payment in Step 2 high and allows for high rebates down the line (Step 5).
“I went to brand manufacturers and said, look, your mission is to sell as much as you can, to help as many people as you can, and by selling at near the list price (versus net price), you’re losing a lot of patients who go without their medications or have to ration their medications because they can’t afford them. People are getting hurt because you’ve taken this business approach. And when I ask them why, they point right to the PBMs,” Mark shares.
“Manufacturers say to me that the PBMs have told them verbatim they will diminish their positioning on their formularies, not just for one drug but for their entire portfolio, if they stop selling to distribution in this manner. That should be illegal.”
PBMs argue that they pass the rebate amount to the health insurance plan, ultimately helping contain costs. Mark has a rebuttal.
“If there was nobody buying that drug, nobody prescribed that drug, there would be zero rebates, right? Because there would be no rebates to give,” Mark prompts.
“So, who effectively is paying for that rebate? It is your sickest employees. It is your sickest employee family members because they’re the ones that have to pay the inflated drug cost during their deductible phase or as a coinsurance or whatever it may be.”
“We are in a system where we allow the PBMs to take advantage of the employers who have an information asymmetry and don’t understand all this stuff, who in turn pass on the cost of the rebates to their sickest employees or family members.”
“That A) should be illegal, and B) is just absolutely batshit crazy. There’s absolutely no logic in that whatsoever. You have this humongous misalignment between the economics and healthcare issues of the patient, the employer, and a PBM.”
Mark has a clear call to action.
“If employers just took the initiative to understand their insurance contract or ran it through Claude or ChatGPT to ask, ‘where are they screwing me over and what should I change in this contract,’ it all would change. But that’s not happening quickly, because the PBMs do everything they can to lie, steal, and cheat from the employers,” Mark explains.
“You see these stories all the time about how the PBMs are being fined by the government or taken to court and losing cases. And people keep on doing business with them. It makes no sense.”
American Employers Overpay for Healthcare
Through quirks of fate and history, 165M Americans have employer-sponsored private health insurance. Because of this, how much American workers pay for healthcare often relies on if their employer’s human resources manager knew what they signed onto on behalf of their company.
“It is not the CEO’s core competency to understand healthcare benefits and costs. They just see it as a line item, even though it’s the second largest expense after payroll,” Mark attests.
Change is challenging. No one wants to go to another all-hands company meeting where they learn that their insurance plan is changing and their kid’s specialist might no longer be in-network.
“Even though the HR people know the system is wrong, it’s the system they know and feel most confident dealing with. The insurance companies know that HR doesn’t want to deal with all that,” Mark evaluates.
Mark coaches CEOs to overcome the friction, noting that any savings from their benefits goes straight to the bottom line. For public companies, these savings can meaningfully increase a company’s market cap or estimated value for investors.
“My job is going around to all these CEOs and explaining to them: you can transition away from PBMs. Because when you think about it, what is it that a PBM does for any employer that somebody else couldn’t do? Nothing. Absolutely nothing.”
“Currently employers are not even allowed to talk directly to Eli Lilly or Novo Nordisk about their GLP-1s because they have to go through their PBMs. That is absolutely crazy, and if you say crazy enough and tell them they’re getting ripped off enough, one by one there will be something that happens that gets them to change,” he predicts.
For employers motivated to make the switch away from their large PBM, Mark has some tips.
“I think that you’re better off going to independent third-party administrators and transparent, pharmacy benefit managers that will allow you to own your claims and audit everything. Those are probably the best starting points,” he advises.
Mark also emphasizes the importance of understanding how benefit brokers or consultants get paid. Some are actually paid by insurers to direct employer customers to higher spend plans. However, any payments must be disclosed in the publicly accessible Form 5500 dataset. Mark advises employers to find someone actually looking out for their best interests, not just trying to inflate costs.
Employers leaning into reforming their benefits can also check out Cost Plus Wellness, an open-source website full of direct employer to provider contracts with transparent pricing deals. Once again, Mark has created a path to savings by cutting out middlemen and favoring transparent, upfront pricing rules.
“I went to hospital CEOs and CFOs and asked what their pain points were with insurance. They said that insurance never paid even the negotiated rates in full and never paid on time. Doctors get stuck with peer-to-peer reviews for insurance pre-authorizations, and even after there are ways to delay care because insurance wants to keep the premiums in their pocket and earn that time value of money. That is a big issue for hospitals,” Mark summarizes.
The stories are egregious. At one point a hospital told him about a patient that insurance had go through 37 different pre-authorizations.
“That’s crazy when you think about the fact that it’s the insurance company that put together the network and picked out the doctors, and they’re now telling you they don’t trust the doctors and hospitals that they picked, so they’re going to deny the claims.”
Simultaneously, Mark assesses that hospitals provide low or interest-free financial assistance payment plans for patients struggling to pay for care that transforms hospitals into subprime lenders.
“Hospitals are getting underpaid, late-paid, payments clawed back, audited, denied, delayed, and have to hire all these administrators and lawyers and revenue cycle management consultants, just to collect the money that they were supposed to get anyways.”
Enter Cost Plus Wellness.
“I said to the hospitals, what if you gave us a good price, maybe not even as cheap as the cash price but a really good price, benchmarked to Medicare. I want the ability to publish the contract that we’re doing on an open-source website because I want other employers to be able to see and say we’d like to do that too. And until you give us reason not to, we are going to trust the doctors and trust the network.”
“Turns out we’ve saved a lot of money. The hospitals are actually making more money from us, which they love, and they’re not having to face pre-authorizations.”
Leaning into the open-source identity, Mark encourages any provider or any employer to join the movement. Most of the contracts on the site currently originate from the Dallas [population: 1.3M], Texas [population: 32M] area since that is where Mark is based. However, this is truly a national issue, so as the movement grows, Cost Plus Wellness will likely expand to encompass the full geographic range of America.
The Biggest Hit Yet: Mobilize Manufacturing
With everything that Mark Cuban is working on in healthcare, you might be wondering what the biggest hit will be. He predicts that it could be what he and his Cost Plus Drugs team are doing in manufacturing, particularly for rare genetic disease therapies.
Spearheaded by Mark’s cofounder Dr. Alex Oshmyansky, the team has deployed AI and robotics in their Dallas Cost Plus Drugs manufacturing facility. They then managed to shrink down the core machinery to fit into a tractor-trailer (aka semi-truck or 18-wheeler depending on where you’re from). The teams call these mobile units their manufacturing pods.
There are three different types of pods: one equipped to manufacture tablets, one to manufacture biologics and biosimilars, and one to manufacture “N of 1” rare disease gene therapies.
Historically patients with extremely rare genetic diseases face monumental barriers to getting effective treatments. Solving the science can remain a hurdle, but there is also an economic reality that pharmaceutical and biotech companies invest their R&D based on revenue opportunity. Ultra small patient populations are often not sufficient for these companies to chase treatments and cures. Families and patient advocacy organizations play an outsized role in championing investment and spearheading biopharma initiatives for these conditions. Within the past few years there have been huge patient successes (like Baby KJ in Philadelphia) and scientific gains. Curative therapies for patients, especially infants, with extremely rare genetic diseases have never been closer. Mark and his team are working to make them even closer – metaphorically and quite literally.
“Unfortunately, you can have tragic cases of a kid who’s one of only maybe 12 people in the world with a genetic disease. They might raise a bunch of money to create the therapy for this child. But the problem is, in order to get it manufactured, you’re going to have some delay waiting for it to be your turn at the manufacturing facility. Because the manufacturing facility wants to maximize their earnings, they’re also going to charge you half a million dollars or more. And it’s going to take at least 6 months, if not a year, to get scheduled,” Mark details.
“We will take one of these pods and park it near the hospital, or the hospital could buy one of the pods so it’s always there and available. We will get that manufacturing cost down to $50,000, and rather than it being 6 months, it could be 3 to 5 months, depending on the complexity. Even more important, because the pod is right there and readily available, if the first therapy doesn’t work and you have to iterate, it’s only $50,000 a pop, and it’s right there, and you can do it as quickly as you possibly can to hopefully help and save somebody.”
“We’ve just started. We have two test cases we’re working on right now. It’s new to the doctors and the scientists, so we’re working to put all those pieces together. But it could be our biggest hit. It could be the most impactful thing that we do, because bringing patients from disease state, to therapy, to cure? That’s huge.”
*****
To hear the full interview recording, visit here
If you are interested in learning more about employer-sponsored insurance, I recommend checking out the Arkansas States of Healthcare Interview with billing expert Kimberly Carleson
If you are interested in learning more about rare disease gene therapies, I recommend checking out the Minnesota States of Healthcare Interview with SMA mom Carolyn Philstrom





Leave a comment